Customization – The gift that keeps on costing
As the saying goes among software industry veterans, the cost burden of a highly customized product is applied to the customer “up-front and over-and-over, every day, inside and outside.”
Hospitals and other companies need to be somewhat aware of commercial software development economics, as it applies to buyers, since they are buying so much IT these days. A software product company does best when the high cost of developing the software is spread across many customers that use the same software as it is. Customization changes that. It requires each customer for which customization is done to bear the distinct and direct costs of that development that is uniquely done for them. There may be ways to economize the process, but it becomes substantial when much of the delivered software is customized. When the Total Cost of Ownership (TCO) for the software customer is considered, as it should be, customization costs becomes a big concern.
That is broken down as:
Up-front – The customer starts paying from contract-signing, before they can even access the product and long before they can really understand what will result from the process and assess its value.
Over-and-over – In that mode, customers usually think up and request additional changes from time to time. That then costs additional project dollars, and changes sometime become a continual process.
Every day – All enhancements that the company routinely makes to its base product must be specifically tailored to the unique version each customer is using. Looking at such effort for all of its customers and the additional overhead of tracking what software changes everyone has, this customization-focused approach, overall, is a more expense way to run the business of the software provider. That ongoing additional expense is reflected in all the pricing and fees the software company charges its customers.
Inside and outside – In addition to the costs paid to the software provider (outside), a significant customization effort requires that the hospital’s own (inside) employees – often some very busy key employees – are required to spend time documenting their needs. They must explain their work to the software companies analysts and review the output of various stages of the custom development lifecycle.
Some may suggest, and others believe, that major customization is the only way to obtain software that users in a variety of hospitals can effectively and enjoyably use in their particular environment, but that is simply not the case. Users don’t customize Microsoft Office applications like Word and Excel but are presented with many options to pick preferences and configuration settings, and provide localization data used by the application. Long term, users and the companies that buy applications come to understand that very particular choices that are applied in major customization efforts don’t really change the value of the use of the application in ways that could not have been done with truly good workflow and user experience design, by professionals, up front. And, overall, the idea that customization is some kind of norm has to be considered in a broader context. What other non-software products that healthcare providers, or the individuals who lead it, buy are customized ? Probably not many because of its being cost-prohibitive when the impact of custom development is considered against what can be achieved with readily available options and configurability.
The long-term, strategic and most insidious cost of customization is the bad habit that it enables among management. Faced with a truly innovative product, which necessarily represents change, leaders and staff in hospitals can, and do, customize their new products back to the familiar appearance, sequences, artifacts (forms,reports, etc.) and activities that they have used for decades, nullifying expertly-designed process innovation. Because that which is familiar is relatively comfortable. Can anyone calculate the total cost of healthcare’s infamous resistance to change ?
The approaches outlined below have earned for our ActionCue® Clinical Intelligence product very high user satisfaction scores, many spontaneous statements of praise and 100% customer retention from its inception. Cost conservation is addressed at every part of the application and our operation. So, it doesn’t mean that we don’t listen to customer input or modify the product for it. We simply are prudent in making changes that truly make the product more valuable and the customer experience more rewarding.
- The application is architected for workflows, calculations, data visualization and ease of use into a turnkey system that is up and running in 48 hours or less after sign-up to begin configuring it for client particulars. Clients are using the application productively within 30 days, and it is similarly very easy to revise as the organization and users assignments change without programmer intervention.
- The design of our pages, workflows, and user interface is designed by a combined team of experts on clinical operations and quality and software functionality, using best practices from both. We apply learning and perceptive psychology techniques to make ease-of-use a reality and a top priority.
- With all customers using the same software, configured for individual needs, it is very easy to deploy enhancements and improvements to the application, which we do every month, with no client/user involvement.
- When customers do suggest changes that Prista has not yet identified, that are valuable and applicable to the majority of our customer base, there is no charge passed along to the customer.
- This streamlined way to producing and deploying changes means that our operation remains efficient and quick to respond.
Tackling the Top 10 Patient Safety Concerns with a Culture of Safety – Part 2
The ECRI Institute recently published their Top 10 Patient Safety Concerns for Healthcare Organizations for 2017. In part 1 of this article, we explored some ways you can target these concerns by developing a culture of safety.
Let’s finish our countdown with the remaining top 5 patient safety concerns for healthcare organizations.
5. Antimicrobial Stewardship
The CDC has been pushing antimicrobial stewardship for quite some time, and it’s still a major issue. We just don’t have antibiotics anymore that can treat bacterial infections because we’ve been abusing them for so long. So, what can organizations do?
The first strategy is to hold subscribers accountable. If physicians are prescribing, we have to hold them accountable and set the guidelines. Some organizations have started with a physician advocate since physicians are more likely to listen to other physicians. Educating patients, families and the general public is important too, as are automatic stop orders.
Once again, leadership from the top is essential in addressing this safety issue. Leadership includes your medical staff and your pharmacist as well. Everyone has to be committed to the outcome and be held accountable. Use your physician peer-to-peer relationship and include your pharmacist as well as your physicians.
Once you have leadership buy-in, work on tracking your safety events. You need to be doing this in real-time, not after the fact or three months later. There’s no point in presenting data to a committee with information that’s so old it can’t possibly be used.
You also need to be tracking your implementation of your processes, including automatic stop orders. Does your pharmacist have a way to report interventions with an automated process that uses one sheet, one entry form and one process? When they click, is all the information they need available? Let technology work for you. Technology should always be one of the action steps that you put in your performance improvement action plans. It’s not just about tracking action tracking. It’s improving so you can take action.
One way to start is with a hierarchy of action steps. We all tend to do the same things over and over again and then wonder why the problem pops up again next year. The National Center for Patient Safety offers a recommended hierarchy of actions, ranging from stronger to weaker actions. Looking at the weaker actions, we can see that often, the only steps we take are about creating a new process. We say, “Let’s just change the policy. Let’s just train everybody, because the problem is always the staff. We have to train them, educate them and coach them.”
This is the wrong approach. Look at the process instead. Weight and monitor your strong actions and see what’s working best at your facility. Take new devices, for example. Do you have a safety event that lets your staff enter near misses and the actual events that happened as a result of equipment? Whether it’s IT, medical equipment or alarms, you want to be able to get those near misses up front so you can identify what needs to be bought. Equipment costs money, and we know how hard that is to get sometimes.
Device use, purchasing and testing is another high strong action plan. Standardizing equipment can be done with new practices and processes streamlined to eliminate redundancy. Engineering control or interlock (forcing functions) allows you to create your systems that can walk you through a workflow process. Workflow processes are great because they lock you out forcing you into the right direction and educating you along the way.
Don’t forget to include checklists. This is a perfect process to use with a mobile device. As you are walking around the facility, you can be looking at information like patient identification and surgical procedures and watching people work in real time. Read back is also critical. Enhancing the documentation and communication is a good weighted action step.
Now that you’re empowered with this information, go back and look at your action plans. Help your staff. Get them excited about really doing something productive. They need to not just be blaming someone but looking at the process.
4. Critical Test Result Reporting and Follow-Up
We’ve been doing critical test results for a very long time, but they’re still a problem because clinicians and departments are still so focused on tasks. You’ve got to get the paper filled out, the order done, the lab drawn and get the test. Then what? What are you supposed to do next?
The first step is to analyze your test process. Have a very specific safety event that doesn’t focus just on labs, but radiology too. All of the accreditation agencies are looking at radiologic testing, and this process has a huge impact from a safety perspective. Have all the steps in the processes and create a report immediately, with a click of the button, and drill down to your problems.
This process can give you a huge return on investment. When you go back to your facilities, you can tell them that you need a process that’s going to give you real-time information, right now, that you can click and filter and drill down into. You need dynamic data, not dead data, so you can get information back immediately and actually analyze and use it.
3. Implementation and Use of Clinical Decision Support
This safety concern is mostly about your EHR. However, while EHR has an important function and is concerned with the care of the patient, decision support is something you can be doing as well. Quality risk is operations. Let’s look at some of the strategies you can use to support your staff.
You’re probably already using physician order entry with protocol orders. But what about flags and alerts? Everybody thinks about putting them in the EHR, but what about in your safety event processes? What about in your quality processes? Do you have a very simple visual way to see exactly what you need to focus and work on?
Visibility and accessibility are very important. Why have data and analysis charts if your staff doesn’t know about them, are the last people to know or are waiting for a paper post to be out on the unit sometime after the committee meeting three months later? You want visibility and accessibility in real-time, with a click of the button.
What about IT and clinical? Although we’re now seeing clinical informatics in facilities, most still rely on history, structure and the way things have always been done. We have to overcome this barrier. We need a workplace focused on performance with quality risk management platform that we can go and use every day as an information management system. That’s a vast improvement over focusing everything on EHR.
2. Unrecognized Patient Deterioration
Healthcare has done a great job over the past several years to really monitor care, including following best practices for stroke, heart attacks and similar events. We need to approach patient deterioration the same way. Rapid response teams worked for a long time, but they seem to have dropped off of the radar. We need to go back to assessing the patients, and that goes back to your nursing process.
Assessing a patient’s risk early is not just a check box on an admission documentation, but a thorough assessment that really identifies the risks for deterioration. Teach your staff more and cultivate their competencies. Redevelop that rapid response team. They need to be able to plan appropriate care for everyone’s individual needs based on that risk assessment. It’s not a standard, with standard vital signs, medications and safety rounds. It needs to be individualized. Use your tools, all those clinical systems that create flags, and use your quality risk management platform too. That’s the one that will give you early warning ideas.
Plan for appropriate care and educate your patients as well. It’s critical to involve the patient in everything you do. Your technical monitoring should be monitoring your practice as well as your patients. You already have compliance checklists for things like sepsis, maternal serious events, clinical bundles, etc., so use all of those. Automate them, put them on a mobile and go around and use them in real time.
1. Information Management in EHRs
Information management is about your EHR, and it’s a great system where everything can be standardized and completed. One thing you should have done immediately when implementing your EHR system was to get your frontline staff involved. One problem you might be facing, however, is turnover. When this happens, new staff members fail to adopt the system because some of them don’t like automation. But that doesn’t mean you should stop tracking.
Here are 10 serious issues still plaguing information management. Some of them have been around for a long time and are not only high-volume problems, but also have the highest potential to cause harm.
- Infusion errors can be deadly if simple safety steps overlooked
- Inadequate cleaning of complex reusable instruments can lead to infections
- Missed ventilator alarms can lead to patient harm
- Undetected opioid-induced respiratory depressions
- Infection risks with heater-cooler devices used in CV surgery
- Software management gaps put patients and data at risk
- Occupational radiation hazards in hybrid ORs
- Automated dispensing cabinet setup and user errors cause medication mishaps
- Surgical staples misuse and malfunctions
- Device failures caused by cleaning products and practices.
Building a Culture of Safety
When all is said and done, a culture of safety is about core values and behaviors resulting from a collective and sustained commitment by organizational leaders and managers in healthcare that emphasize safety every day.
Every day when your staff walks into the facility, safety should be priority number one. Let’s all do the safety dance, because that’s what it’s all about. Make it fun every day. It’s not a drudgery, but something we need to do for each other.
Tackling the Top 10 Patient Safety Concerns with a Culture of Safety – Part 1
The ECRI Institute recently published their Top 10 Patient Safety Concerns for Healthcare Organizations for 2017. Several of these items were on last year’s list, which means we in healthcare still have work to do to drive improvement and meet targeted goals.
Aside from just highlighting new and recurring safety concerns, this list is also a great starting point for inspiring patient safety discussions and setting priorities in your own organization. Here are some ways you can target these concerns by developing a culture of safety.
Let’s begin by counting down, David Letterman style, from ten to one. Since there is much we can say about each finding, we will be covering only 5 safety concerns in this article and the remaining 5 in a second article.
10. Inadequate organization systems or processes to improve safety and quality
There are numerous studies that link error prevention to a culture of safety—being proactive and setting strong preventive strategies rather than waiting for patients to be harmed. This is such an important issue that the Sentinel Event Alert recently addressed the essential role of leadership in developing a safety culture.
Unfortunately, healthcare has been very slow to adopt a culture of safety. Let’s take a look at exactly what a culture of safety is and how leadership is essential to creating one in an organization.
What is a “Culture of Safety”?
Safety cultures have been around a long time, but they’ve only recently been adopted in healthcare. High-reliability organizations are committed to safety by consistently minimizing adverse events at all levels, from frontline providers to managers and executives. This commitment establishes a culture of safety built around the following 7 pillars:
- Leadership
- Teamwork
- Evidence-based
- Communication
- Learning
- Just culture
- Patient-centered
If you’ve been with The Joint Commission and several of the accreditation agencies, you know that leadership has always been first. We kind of take it with a grain of salt, but we can’t anymore. Leadership has to be the most important thing that happens.
The drive needs to start from the top and involve more than executives just putting a stamp on the policy and the plan. Leadership has to own a culture of safety, and when they own it, the team owns it.
Getting real, evidence-based data helps with the communication and the learning of your team members. Leaders have to support a just culture of learning rather than blaming and balance individual accountability with organizational responsibility.
Finally, a culture of safety needs to be patient-centered. You need to include the community and the patients in everything that you do.
9. Management of New Oral Anticoagulants
Tracking adverse events for anticoagulant drugs for has been a part of safety reporting for years, but four new oral anticoagulant medications have been approved since 2014. Here are some strategies and questions you may want to consider when managing these new additions.
Standardized order sets based on individual’s indications
Are you using standardized order sets? Maybe it is time to review to validate if they are evidence-based and individualized.
CDS to alert practitioners to duplication of therapy
Do you have clinical decision systems that can alert your practitioners about duplications or errors in protocols? Having flags on your systems is critical.
Multidisciplinary team plans for reversal of anticoagulant therapy
Consider a multidisciplinary approach to assessing, monitoring and treating for reversal of therapy. Break down the silos that have been around too long.
Reversal agents should be readily accessible
What compliance process measures are you tracking? Are the effective in getting you the information you need to improve? In ActionCue CI, we have a measure for tracking Reversal Agent Usage. This is an example of error prevention, analyze and assess where the problems are and fix it.
Collection and analysis of events
Collection and analysis of events is what ActionCue CI does well. Let’s go one step further and take action for improvement.
8. Inadequate Management of Behavioral Health Issues in Non-Behavioral Health Settings
Behavioral health hospitals have been doing this for quite some time, but healthcare hospitals are not as good at recognizing a patient’s behavioral health. It’s essential that you start preventatively tracking behavior before it becomes a norm in the environment. When you do that, you get outcomes that you can analyze and prioritize.
Your tracking system should include clinical as well as unsafe environment special events. ActionCue CI gives users a Behavior event category training staff to be competent on identifying, reporting and resolving issues. One event ActionCue CI tracks is rapid response. Train your staff now to be competent on identifying those issues, early signs and behavior cues. Don’t wait until it gets to be serious.
7. Opioid Administration and Monitoring in Acute Care
This is a serious situation in this country, not just in acute care. You want to track all of your rescue drug and narcotics usage. But how? Are you looking at narcotic adverse drug events? What’s your reversal drug rate? How many times have you had to use your reversal drugs and for what reasons?
You also need to look at your protocols. What are your protocols for rapid response? Do you have the right equipment? Do you need to buy new equipment? You need to be looking at your medical equipment to make sure it’s up to standards.
Finally, you need to look at the nursing process as you’re investigating events and recommending solutions. You need to go back to look at the basic process so that you’re not forgetting anything as you’re assessing.
6. Patient Identification
Many healthcare settings have stopped tracking patient identification errors. But when you consider that out of 7, 613 events, 9% resulted in patient injury, including two deaths, this is still a serious issue that needs to be addressed from the leadership down.
Leaders can start by fully supporting patient identification initiatives by prioritizing the issue, engaging clinical and nonclinical staff, and asking staff to identify barriers to safe identification practices.
Go back to tracking your patient identification and include in your policies and procedures the contributing causes to the problems the team identified from the event reports. Make this something in your investigation process that your staff are looking at. Your end users are your best value. They’re the ones who see everything that’s going on and who know what needs to be fixed. Give them the opportunity to be involved.
Imagine if you had a button in your event that would automatically create a performance improvement action team. Let’s say the safety risk manager sees that this is the fifth time he’s seen patient identification as a problem. With the click of a button, he decides to create a team. The team works from within the application which serves as a working platform so they can collaborate. Reports are generated automatically, which include the month-to-month analysis and compares agencies and experts that you want to compare yourself to.
The best thing, however, is that you also get the action plan attached to a scorecard report and run chart in ActionCue CI. This is created in real time so you don’t have to wait. It’s all about efficiency. Why should a quality manager go to a committee meeting, decide that she needs a team and spend 2-4 weeks getting one together? She should be able to have the information she needs at her fingertips that she can drill down into.
Focus on the Process
It’s difficult and unsustainable to cram everyone’s head so full of education to the degree that they will continually act in a heroic manner to overcome flaws or deficits in institutional processes and leadership. Until we focus on optimizing the work itself with best process innovations, technology, leadership, goals and respect, organizations will “keep on getting what they’ve always got,” which is not the culture of safety we all need.
In part 2 of this article, we will review the remaining top 5 patient safety concerns for healthcare organizations as they apply to our focus on building a culture of safety.
7 Steps to Increasing ROI with Performance Improvement
For a long time, Quality and Safety Event reporting have been recognized as important but often downplayed tasks when it came to getting the attention of executives and allocating resources. Shifting investments and allocating resources has become even more of a challenge as budgets continue to get tighter and tighter.
Quality-related reimbursement, as applied through Value-Based Purchasing (VBP), MACRO/MIPS, ACO programs and other components in the pay-for performance (P4P) model, have only increased the pressure without providing much guidance on how to actually improve quality.
Although the goal of submitting quality and safety reports and data to external organizations is becoming something more than just checking a “to-do” item off the list, much of the reporting and education efforts in hospitals and other healthcare organizations fall short of making real advancements in Performance Improvement.
The ROI that can perk up executives’ attention and guide their investment is to make Performance Improvement more effective and efficient. While Performance Improvement has been a focus for decades, most organizations focus on the wrong things, such as manually gathering information and data and over-educating staff on the theories and science of QI methodologies. Others are still wasting their time with more meetings, more documents and artifacts and more working overhead.
Worse still, all of these efforts suffer negligible support from innovative IT solutions that are specifically designed to support more efficient and effective Performance Improvement. This is the year, maybe even the quarter, to change that.
Start from the Top
Championing the shift from investing in reporting to investing in the Performance Improvement process itself has to come from the top. Senior management up to the C-suite needs to not only lead, inspire and set the direction, but also provide the resources and fully communicate the importance of creating a smarter and more efficient Performance Improvement process.
Instead of merely asking staff and managers to just “work harder and better,” the goal needs to be about making their job easier and more streamlined.
7 Steps to Better Performance Improvement
An efficient Performance Improvement system needs to be supported by innovative and intuitive IT and can be achieved by taking the following steps.
- Abandon historically-rooted inefficiencies, including artifacts and activities of decades-old QI programs, functional and organizational boundaries that disrupt workflows and manual data gathering and processing.
- Get everyone on the same page with tools that integrate improvement, all quality metrics and event reporting/investigation.
- Ensure every internal reporting and analytic activity drives into improvement.
- Focus on enabling the improvement work correctly instead of over-educating the staff.
- Prioritize synergistic, internal, real improvement activities over external reporting.
- Make sure the access and presentation of needed insight for executives is just right—not too deep and complex nor too shallow and impenetrable—so they can own and drive the effort appropriately.
- Implement a technology-enabled PI workbench specifically for improvement efforts that does all of the above, streamlines and offloads manual efforts from staff and leaders, delivers results and ROI and supports a real culture of improvement in quality and safety.
Improving ROI with Technology
Each of these steps has the potential to be a project in its own right and a daunting task at that. Fortunately, a growing awareness of how Performance Improvement and Quality and Safety reporting can feed one another is prompting a shift in technologies and platforms to support this new focus.
ActionCue CI was built intentionally to increase ROI by changing how Performance Improvement is managed and facilitated using the steps outlined above. Learn more about how ActionCue can help executives, risk/quality managers and clinical staff bring Performance Improvement into the 21st century.
Flu, pneumonia deaths exceed epidemic threshold
Becker’s Healthcare reports statistics on a significant rise in influenza and pneumonia deaths, focusing on flu-related death in 10 states: Alabama, Georgia, Kansas, Louisiana, Minnesota, Missouri, New Jersey, Oklahoma, South Carolina and Tennessee.
With such outcomes, the tracking of clinical staff immunizations, according to guidelines, becomes critical to impact the outcomes as well as for compliance reasons. As with many standards, being compliant needs at least as much focus by healthcare management as reporting compliance. How well is your healthcare delivery organization doing at its part in containing influenza, pneumonia and other diseases through vaccination efforts ?
Our research shows that the most successful vaccination programs have good operational tracking that:
- is particularly easy for capture or entry of vaccination data
- is structured to match the reporting requirements as to demographics and disposition
- provides no-hassle reports that are very accessible, easy to interpret and focused on action for staff, managers and executives
- is institutionalized so everyone is aware and on the same page
ActionCue Clinical Information has built-in forms for CDC/NHSN-defined data requirements and a built-in report with both detailed data and immediate indication of immunization program effectiveness.
Form for easy entry of disposition data
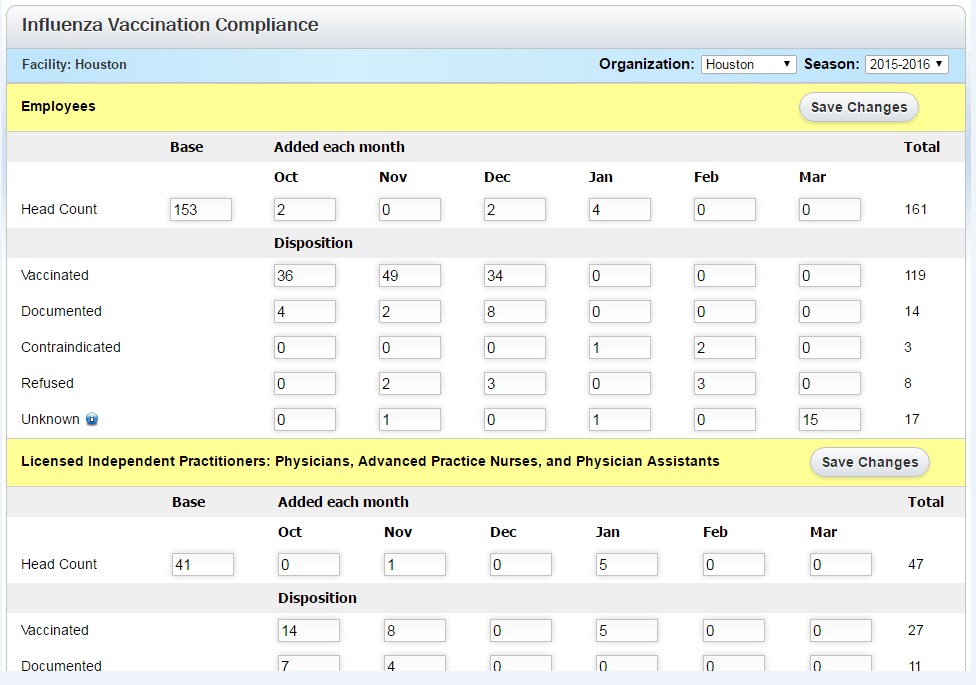
Built-in Report

ActionCue CI saves clinical managers 20-30% of their work time while delivering more insightful, actionable information across the entire Quality, Patient Safety and Performance Improvement effort. Over 90% of organizations using the ActionCue application are compliant with vaccination requirements and compliance is just that clear.